Select your local website





















|
How VAP develops |
Problems caused by VAP |
| ||
 |
 |
|||
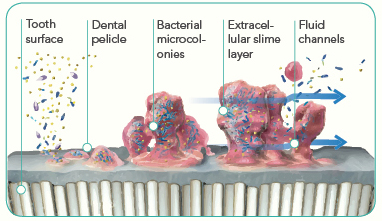
| Ventilator associated pneumonia (VAP) causes prolonged intubation and a prolonged stay in ICU with the associated costs. It is also a serious cause of mortality in compromised patients. 1,2,3,4 Dental plaque is a biofilm made up from bacteria and their excretions. At home we are not concerned about it, as actions such as eating and speaking help remove this film. In ICU patients are exposed to many different bacteria than what is found in our homes: MRSA, Acinetobacter, Klebsiella or other potentially lethal bacteria may colonize in the warm and humid oropharyngeal environment. Dental plaque is mostly located on the gum line and in-between the teeth. Using gauze or a sponge will not remove these bacteria. A soft brush with slightly longer bristles is ideal to remove plaque from inter-dental spaces. Use the modified Bass brushing technique and don’t put any pressure on the gums. This will ensure proper removal of the plaque film. It is important to break up this film prior to applying antibacterial solutions, as bacteria inside the biofilm are protected. |
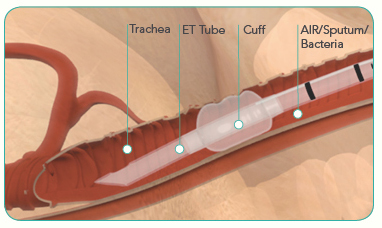
If plaque and bacteria are not removed, they will drain down to the ET tube cuff. Since the cuff seal is never 100%, aspiration pneumonia can occur and VAP will develop. It is important as part of the oral care protocol to suction out the space above cuff regularly in order to avoid aspiration of bacteria into the lungs. VAP develops is 9-25% of all patients in ICU. Each case of VAP may cost the hospital as much as $30,000-$40,000. It is therefore in the best interest of each hospital to reduce their VAP rates and associated costs. VAP is also one of the highest causes for morbidity and mortality in ICU, with mortality rates as high as 10-40%. |
|
Background |
Procedures |
Tools | ||
Bacteria found in ICU are different from those at home therefore the same brushing habits which are used at home do not apply to a patient in ICU. The bacteria, which are responsible for plaque in ICU, may include Staphylococcus aureus (including MRSA), Burkholdia cepacia or Acinetobacter species. These may cause a serious problem for the patient in ICU. Plaque, a bacterial biofilm, builds up very fast covering the complete tooth surface in as little as two hours. The Center for Disease Control (CDC) in the United States are therefore recommending an oral intervention every two hours to reduce the incidence of VAP. |
The best product to remove plaque is a tooth brush with soft bristles. This will effectively remove the plaque on the surface and the interdental spaces. It is recommended to use a brush at least twice a day. For patients with extremely sore gums, patients without teeth or those who require less traumatic oral care during the day, a soft suction swab or oral suction wand is sufficient. Mouth rinses, medicinal or cosmetic, may also be used in conjunction with the hospital oral care protocol. Mouth care should always finish with a lip moisturiser such as vaseline or an antibiotic prescription gel which may be applied with a soft sponge. To remove secretions around the ET tube cuff, where most of the micro-aspirations occur, use a soft oropharyngeal catheter which is specifically designed for this application. |
Hospitals are recommended to develop their own protocols for the control and reduction of VAP in ICU. An oral care programme is part of this and can be part of a ventilator care bundle. The frequency and required tools will be determined by the current VAP rates, infection control requirements, available personnel and other issues. It is recommended that all patients first are assessed for their oral status and the actual procedures then should be documented for each patient. We offer an assessment chart and protocol in our evidence section to provide you with a guide but these should be adjusted for the individual hospital requirements. |
Recommended brushing technique
|
The modified Bass brushing technique |
 |
| ||



References
[1] : C.A. VAN NIEUWENHOVEN, E. BUSKENS, D.C. BERGMANS, F.H. VAN THIEL, G. RAMSAY et J.M. BONTEN, Oral decontamination is cost-saving in the prevention of ventilator associated pneumonia in intensive care units, 2004.
[2] : R.F. ABIDIA, Oral Care in the Intensive Care Unit : A Review, The Journal of Contemporary Dental Practice, Volume 8, No. 1, January 2007.
[3] : R. GARCIA, A review of the possible role of oral and dental colonization on the occurrence of health care-associated pneumonia: Underappreciated risk and a call for interventions, AJIC, November 2005.
[4] : R. GARCIA, L. JENDRESKY, L. COLBERT, A. BAILEY, M. ZAMAN et M. MAJUMDER, Reducing Ventilator-Associated Pneumonia Through Advanced Oral-Dental Care: A 48-Month Study, AJCC, July 2009.
